Pavilion Publishing and Media Ltd
Blue Sky Offices Shoreham, 25 Cecil Pashley Way, Shoreham-by-Sea, West Sussex, BN43 5FF, UNITED KINGDOM
Tel: +44 (0)1273 434 943
Email: [email protected]


In the excitement of planning a trip abroad, health precautions are often the last consideration of travellers. Late business trips and the easy availability of online booking of last-minute foreign holidays add to the problems of the travel health adviser faced with a traveller who is departing in a few days’ time.
Some travellers may have only a hazy idea of the geographical location of their destination, while health information is not usually very prominent or even accurate in their booking information. Is it then possible to give adequate advice and help to these travellers?
Key points
|
Travel health advisers need to have some knowledge of the location, topography and climate of the countries to which their travellers are going. As well as medical books in the practice library, a good world atlas is invaluable.
The length and nature of the proposed trip, the likely activities to be undertaken and the budget and type of accommodation to be used are all important factors in assessing the traveller’s health risks and the precautions likely to be needed.
Connection to an online database such as Travax (www. travax.nhs.uk) is essential to assist in building up the individual risk assessment for each traveller, whatever the time-scale of his or her travel.
For travellers with a vague itinerary, it is better to plan for the worst possible case scenario and act accordingly. For example, if there are different levels of malaria risk in different areas that might be visited, it is wise to prescribe prophylaxis that will cover the risk in the highest risk area and to prescribe the same antimalarial drug throughout the whole trip.
Particularly in the case of backpackers and low-budget travellers, it is wise to assume that if there is a possibility of a health risk they should be protected against it wherever possible. Other high-risk groups are those likely to be living and mixing at close quarters with indigenous people in developing countries and sharing similar standards of food, water, infrastructure and accommodation to which package tourists are not normally exposed.
Vaccines may take up to 2 weeks to provide optimum levels of protection, though reinforcing (‘booster’) doses following an earlier primary vaccination become effective more rapidly. For this reason, it is worth giving reinforcing doses of vaccines in the UK child immunisation schedule, such as tetanus and diphtheria, (if indicated), to last-minute travellers. The decision on whether to offer vaccination to last-minute travellers will depend on a number of considerations.
For very short trips the traveller may be on their way home before the vaccination has become fully effective, though some measure of protection may be obtained. However, for longer stays abroad, necessary vaccinations should still be given even though the early days may be less well protected. It will be necessary for the GP to weigh up the level of risk against the length of the trip and the speed of onset of protection.
Vaccination should always be subject to an individual risk assessment. The last-minute traveller is no exception. For example, a backpacker going to India is at much higher risk from typhoid than a business traveller staying in five-star hotels, and the backpacker’s trip is likely to be longer. Thus, the backpacker should still be vaccinated against typhoid even if he intends to travel tomorrow, whereas business travellers are less likely to be exposed to typhoid and, if their trip is relatively short, the balance is probably against giving the vaccine.
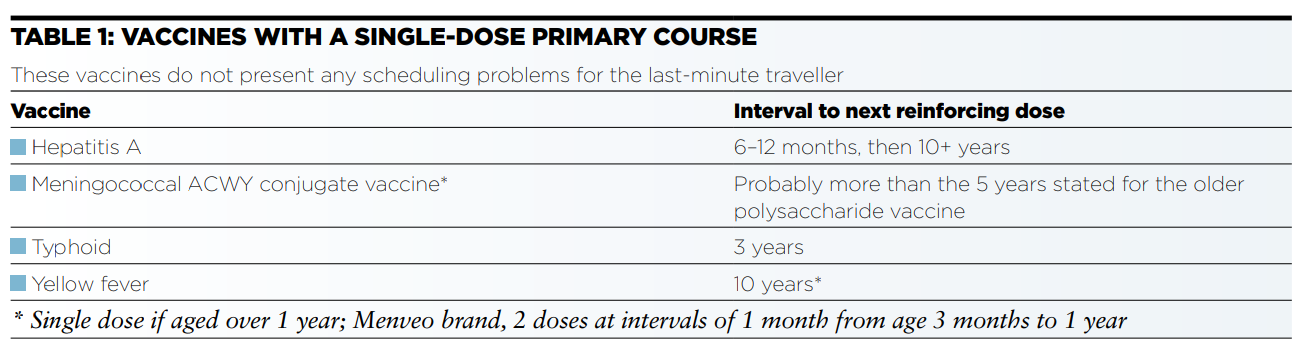
Yellow fever is the only vaccination for which a vaccination certificate is statutorily required for entry to some countries. Even if a certificate is not an entry requirement, it is important that travellers exposed to a risk of yellow fever should be protected as the disease carries a high mortality rate. Protection will be incomplete, and the certificate does not become effective, until 10 days after vaccination, so entry is likely to be refused within that period if it is a statutory requirement.
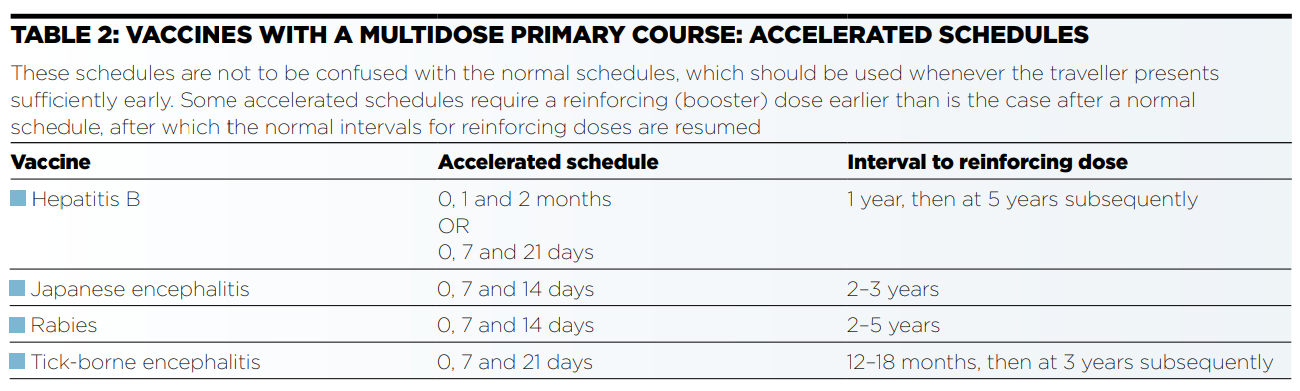
Some vaccines, such as hepatitis B, may be given in an accelerated schedule, e.g. 0, 1 and 2 months or even 0, 7 and 21 days instead of 0, 1 and 6 months (Table 2), but even this schedule may be too long for the last-minute traveller to complete. Initial doses of such a course will confer some degree of immunity while subsequent doses are intended to maintain this immunity for a longer period. For a relatively short-stay traveller, it may therefore be advisable to give as many doses as possible, even if this is only one dose. The course can then be completed on the traveller’s return against the possibility of future exposure to risk, and a primary course can be resumed where it was left off. If the usual schedule is interrupted, it is not necessary to start a primary course again from the beginning. For longer stays it may be possible, depending on the destination, to arrange to have the course completed during travel.
Vaccinations are not the only way of preventing infection. Attention to food, water and personal hygiene, avoidance of insect bites and safe sexual practices will help to protect against many travel-related infections. Leaflets on these topics will help to reduce the amount of verbal information given (and probably forgotten) in what is likely to be a rushed last-minute consultation.
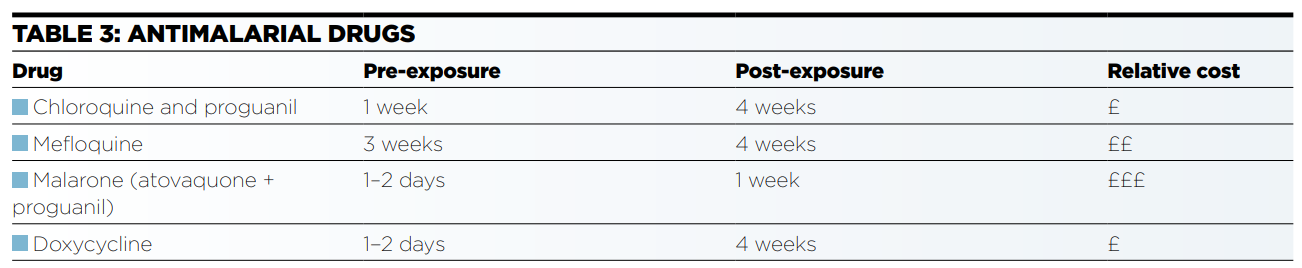
Antimalarial drugs need to be started before travel. Chloroquine and proguanil must be started a week prior to exposure to risk. Mefloquine should be started 3 weeks prior to exposure, as its adverse effects are most likely to be observed in the first 3 weeks; an alternative drug can be chosen, if it proves unsuitable. However, this makes mefloquine less suitable for last-minute travellers.
Very last-minute travellers may use Malarone (atovaquone/proguanil), which can be started 1–2 days prior to exposure, though it is more expensive, and budget travellers may be reluctant to take it. Doxycycline should also be started 1–2 days before exposure and is less expensive. (see Table 3).
If the traveller is going to a high-risk area, it is advisable to start prophylaxis with an appropriate drug, even if the initial period prior to exposure cannot be observed, rather than not taking the drug at all.
Travellers still need to take appropriate anti-bite precautions whatever the situation regarding medication. If they are likely to be exposed to infections transmitted by daytime-biting mosquitoes, such as dengue, they need to observe these precautions during the day as well as between dusk and dawn. Although chemoprophylaxis will still be necessary, the risk of malaria can be reduced by anti-bite precautions, such as:
Time is likely to be at a premium at the last-minute travel consultation. However, these travellers still need advice about health risks, such as food and water, heat, sunlight, accidents, insect bites, etc. The travel health adviser should have a series of leaflets available covering nonvaccine preventable health risks.
It is better to avoid last-minute problems than to have to try to cope with them. Some of the ways in which this could be achieved include:
Online resources
|
This website uses cookies to improve your experience. We'll assume you're ok with this, but you can opt-out if you wish. Accept Read more ...