Pavilion Publishing and Media Ltd
Blue Sky Offices Shoreham, 25 Cecil Pashley Way, Shoreham-by-Sea, West Sussex, BN43 5FF, UNITED KINGDOM
Tel: +44 (0)1273 434 943
Email: [email protected]


Rational pharmacological intervention is essential for optimising glycaemic control in patients with type 2 diabetes. Metformin is the recommended first line agent, but the progressive pathogenesis of type 2 diabetes generally dictates the need for concomitant use of other drugs. Here, Caroline Day discusses the options following metformin monotherapy.
Rational pharmacological intervention is essential for optimising glycaemic control in patients with type 2 diabetes. Metformin is the recommended first line agent, but the progressive pathogenesis of type 2 diabetes generally dictates the need for concomitant use of other drugs. Here, Caroline Day discusses the options following metformin monotherapy.
The pathophysiology of type 2 diabetes dictates that worsening glycaemic control be addressed with agents that provide complementary mechanisms of action which target the underlying lesions. Metformin and sulphonylureas have been the mainstay of treatment for over 50 years and until the 1980s sulphonylureas were the preferred first line therapy. The Universities Group Diabetes Program (UGDP) raised questions regarding the cardiovascular safety of sulphonylureas, and mechanistic studies on metformin showed that it had insulin sparing actions – notably enhancing hepatic insulin sensitivity and offering some improvement in glucose uptake by muscle.1,2
A particular advantage of metformin was that it did not cause weight gain, and the benefits of metformin as first-line therapy in overweight patients in the UK Prospective Diabetes Study (UKPDS) culminated in its current positioning in diabetes treatment algorithms worldwide.2,3 The long term benefits of use of metformin and achieving good glycaemic control early in the course of type 2 diabetes were endorsed in the 10 year UKPDS follow-up study.4
The American Diabetes Association/European Association for the Study of Diabetes (ADA-EASD) consensus published last year (Figure 1) maintains the position of metformin as first-line treatment of choice, although the current consensus – including NICE guidance – acknowledges the benefit of starting
treatment with diet/lifestyle strategies in patients who are close to target and likely to respond to this approach.5,6,7 However, metformin is recommended as an initial treatment in combination with lifestyle changes in those less likely to be adherent, while in those with greater hyperglycaemia (HbA1c 9-10%, 75-86 mmol/mol) commencement of treatment with metformin and another oral glucose lowering agent is recommended. Patients with severe hyperglycaemia (HbA1c >10%; 86 mmol/mol) should be initiated on insulin therapy alone or in combination with other glucose-lowering agents.
Since the publication of the latest consensus a new class of oral glucose lowering agents has been approved in Europe – the SGLT2 inhibitors. The first-in-class agent dapaglifozin has been added to the summary algorithm herein (Figure 1), but it has yet to be included in any official guidelines.
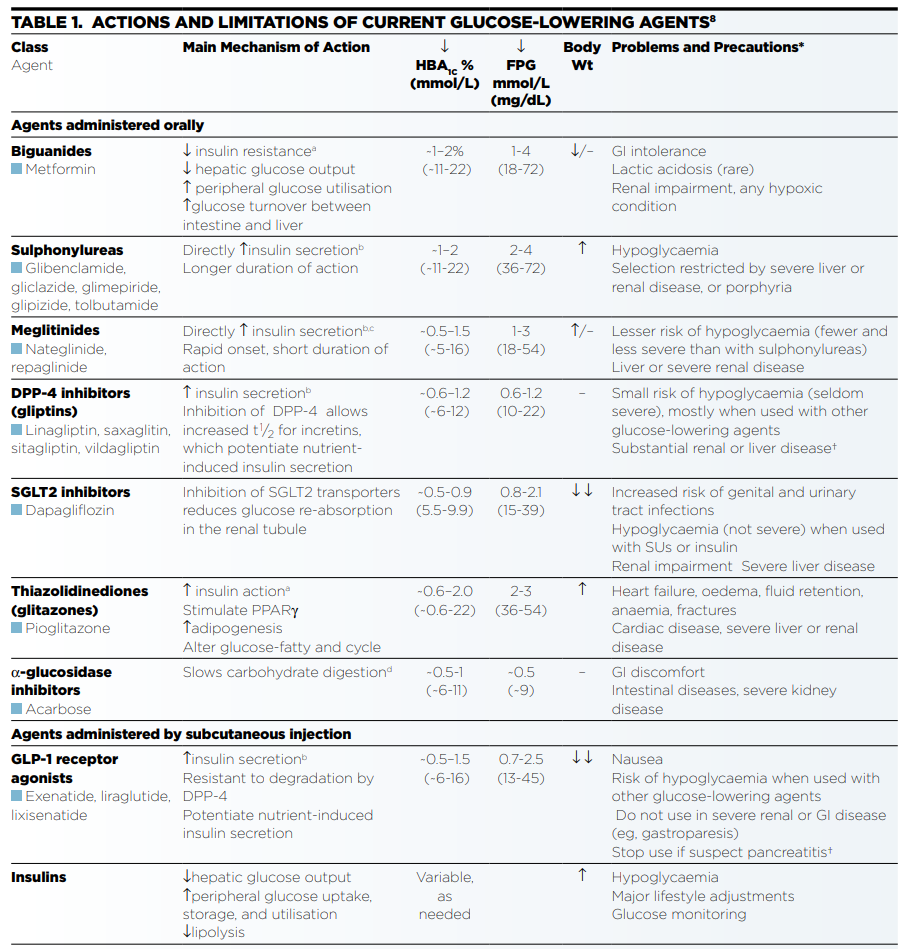
Since 1997 the antidiabetic drugs arena has burgeoned with the advent of the thiazolidinediones (of which only pioglitazone is now available in Europe), the DPP4 inhibitors (gliptins), the injectable GLP-1 receptor agonists, novel insulins and now the SGLT2 inhibitor dapaglifozin. The main feature of glucose lowering agents available in the UK are summarised in Table 1.8
At diagnosis of type 2 diabetes, insulin resistance is already well established and unlikely to diminish unless there is considerable weight loss and an increase in physical activity (to reduce insulin resistance and improve insulin sensitivity). The compensatory hyperinsulinaemia which characterises the pre-diabetic period is diminishing as beta cell failure supervenes, and at diagnosis beta cell reserves maybe so depleted that insulin therapy is needed – thus a patient with
HbA1c >10%, 86 mmol/mol, at diagnosis is unlikely to achieve or maintain adequate glycaemic control without insulin.5
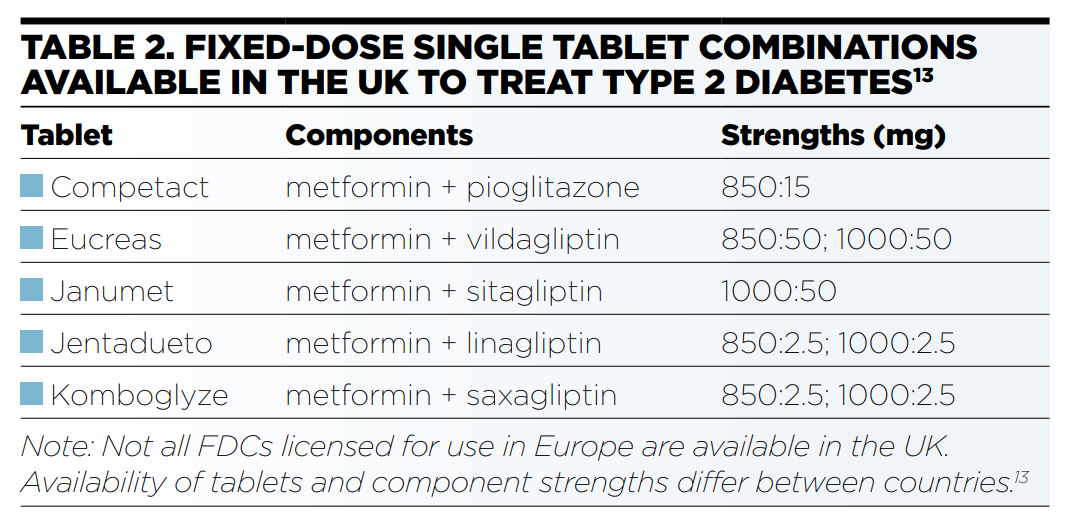
The mechanisms of action of all the glucose lowering agents are complementary to those of metformin, thus the selection of the combination drug to be added in should be individualised. The advent of fixed-dose combination (FDC) tablets should aid adherence. For example, in patients new to combination therapy adherence was not compromised in those initiated on an FDC, and was ~20% better than those on co-administered metformin and glibenclamide.11,12 Several FDCs are used in the USA and many have been approved in Europe, but only those listed in Table 2 are available in the UK.13
People with type 2 diabetes are not as simple to treat as an algorithm would suggest. They tend to be older, have other components of the metabolic syndrome, such as hypertension and dyslipidaemia, and are often on multiple medications to reduce cardiovascular risk (as primary or secondary prevention), or to treat other diabetes-associated conditions as well as other chronic conditions and intercurrent ailments. Ageing brings reduced physiological efficiency, some aspects of which may be of individual importance. Thus the choice of which drug to add to metformin therapy essentially depends upon the individual being treated. The case study below illustrates the case of Mr R.
Case studyMr R, a married 55 year old bus driver of African origin was diagnosed with hypertension 4 months prior to presenting complaining of lethargy, thirst, nocturnal polyuria. He was obese (BMI 32), +ve for urinary protein, his blood pressure 137/80 mmHg (treated with amlodipine 10mg od). Blood analysis revealed total cholesterol 6.5 mmol/L, urea 6.1 mmol/L, creatinine 114 .mol/L, and a random finger stick glucose 24 mmol/L. Mr R was given diet and lifestyle advice and commenced on metformin (500mg od titrated to tds). Simvastatin (20mg od) and aspirin (75mg od) were prescribed to address his increased CV risk, noting the reduced dose of simvastatin due to amlodipine therapy. Despite compliance with his treatment, some of his troubling symptoms persisted, and glycaemic control remained inadequate (fingerstick glucose 14mmol/L). Mr R was agreeable to increasing his medication in an effort to improve his glycaemic control, but stressed that he didn’t want to take any medicines which might compromise his work situation. Although he had ‘come out’ at work he was fearful of his treatment jeopardising his job. Thus treatment options were limited to those which would not cause hypoglycaemia (i.e. avoid suphonylureas and insulin). Mr R admitted that his diet was generally low in complex carbohydrates – deleting acarbose as an option. Due to shift work and bus schedules his eating patterns were unpredictable (timing, quality and quantity) – discounting addition of a meglitinide. Media scares surrounding the TZDs eliminated consideration of pioglitazone. He expressed an interest in taking a GLP – 1ra as he had read online blogs praising the drug for helping them to lose weight. His enthusiasm evaporated when he realised it was only available as an injection; he didn’t want the hassle of using a needle, even if only once a week, if he could take a tablet. Mr R’s managementIn attempting to select an add-on therapy that would be appropriate to Mr R’s work situation and preference (to encourage adherence) therapeutic options were limited to use of a gliptin (DPP-4 i) or glucuretic (SGLT2 i) as neither is associated with hypoglycaemia or weight gain. Mr R had been a regular drinker but since having a bout of pancreatitis 10 years ago he now only had a drink at special events such as weddings. However this raised a caution with regard to prescribing a gliptin. Thus it was decided that Mr R would commence treatment with add-on dapagliflozin (10mg od). It was explained to him that it is a new type of agent, so we would like to see him more regularly than if he was taking a drug for which there is extensive clinical experience. He was also advised that some people had experienced more urinary tract and genital infections when taking this drug. Nevertheless, he was keen to try the new agent – essentially because of its potential to help with weight loss. |
Sulphonylureas are generally accepted as initial choice of add-on therapy to metformin as, provided there is adequate beta cell function, the addition of a sulphonylurea allows patients to rapidly achieve glycaemic targets. However, sulphonylureas are associated with hypoglycaemia and associated risks such as falls, and it has been suggested that fear of hypoglycaemia reduces compliance. The use of add-on meglitinide treatment offers rapid-onset and very short duration of insulinsecretion which reduces risk of hypoglycaemia and these agents are not associated with weight gain. Addition of a DPP4 inhibitor offers similar benefits with the benefit of once-daily dosing (with the exception of vildagliptin which is bd).
Pioglitazone remains a useful agent, particularly in patients who are very insulin resistant, but its associated cautions – e.g. bone fracture and bladder cancer risk – may restrict prescription, particularly in older people.16 Targeting of the incretin system is more direct with GLP-1 receptor agonists, which offer a choice of injection regimen (bd, od or qw) and have the advantage of enhancing weight loss. However, some patients are unable to tolerate drug-related nausea. Observations, mainly from the USA, have generated interest in a possible link between long-term use of incretin-based therapies and a small increased risk of pancreatitis, pancreatic duct metaplasia and pancreatic alpha cell hyperplasia, but a causal effect has yet to be established.14,15
The newest addition to the add-on-to-metformin list is dapagliflozin with its novel non-insulin dependent glucuretic mechanism of action which aids weight loss (but might increase risk of genital and urinary tract infections) while the oldest conventional treatment for diabetes – insulin – may be necessary to achieve adequate glycaemic control. The pros and cons of insulin therapy are well rehearsed, but the range of insulins with different onsets and durations of action and improved insulin delivery devices allow for individualisation of regimens while insulin dosages are reduced with concomitant use of metformin. Indeed a recent retrospective cohort study using data from 84,622 type 2 diabetes patients on the UK General Practice Research Database (GPRD) showed that adverse events and mortality were higher in patients on insulin monotherapy than those on insulin plus metformin.17
Due to metformin’s unique mechanism of action and lack of interactions with other glucose-lowering agents, it is possible for any of the other classes of glucose-lowering agents to be added to metformin therapy. However, such is the nature of type 2 diabetes that dual therapy may not achieve adequate glycaemic control and it might be necessary to add in a third agent with yet another mode of action (additional caution is required as the contraindications to all three agents must be observed).5 The benefits of good glycaemic control as early as possible in the pathogenesis of type 2 diabetes is well established, as is the need to tailor targets and individualise medication strategies and healthy living advice to the personal circumstance of the patient.4,5,18
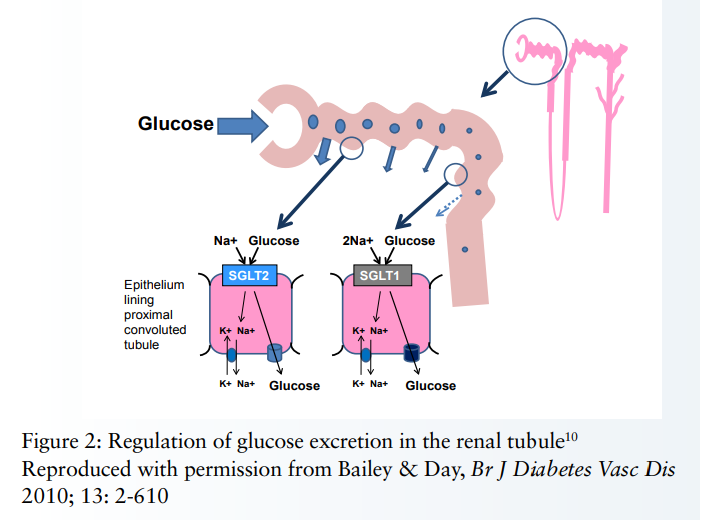
Sglt2 inhibition: a new paradigmIn November 2012 the selective reversible SGLT2 inhibitor dapagliflozin was granted marketing authorisation in Europe for use in type 2 diabetes patients inadequately controlled with lifestyle strategies alone or in combination with other antidiabetic agents, including insulin – although studies on dapagliflozin in combination with a GLP-1ra (glucagon-like peptide-1 receptor agonist) have not been reported. Dapagliflozin as monotherapy is only considered in patients in whom metformin is inappropriate. Dapagliflozin acts by inhibition of SGLT2 transporters. These are located almost exclusively in the renal proximal tubule where their role is to reabsorb glucose back into the circulation.
Thus their inhibition has a glucuretic effect which reduces hyperglycaemia (~0.8% HbA1c) without causing hypoglycaemia, facilitates weight loss (~3kg) via urinary calorie loss, and the small osmotic diueresis is associated with small reductions in blood pressure (~4-5mmHg). The efficacy of dapagliflozin is dependent upon an adequate rate of renal perfusion, and is therefore not recommended for use in moderate renal impairment (i.e. creatinine clearance <60ml/min or eGFR <60ml/min/1.73m2). The presence of SGLT1 transporters in the distal regions of the tubule ensures that there is adequate glucose reabsorption, thereby avoiding hypoglycaemia and neuroglycopenia. It is indeed paradoxical that with SGLT2 inhibitor therapy, glucosuria is an indicator of drug adherence, raising the conundrum of ‘good glucosuria’ and ‘bad glucosuria’.9,10 |
Dr Caroline Day, Visiting Fellow, School of Life and Health Sciences, Aston University, Birmingham.
This website uses cookies to improve your experience. We'll assume you're ok with this, but you can opt-out if you wish. Accept Read more ...